Holistic Tonal Assessment – A Model for practicing Bowen Therapy.
(Article published in the Journal of the Australian Traditional Medicine Society – September 2025)
Katrina Pennington B App Sc (OT) M App Sc (Acupuncture)
Graham Pennington N.D. Grad Dip App Sc (Acupuncture)
ABSTRACT
This article discusses tonal asymmetry as an adaptation to spinal and cranial dysfunction and examines the use of holistic tonal assessment as a tool to guide and prioritize the application of Bowen therapy. The authors introduce the concept of the ‘Window of Symmetry’ and outline its clinical value in helping to transition patients from a state of dysfunction and adaptation to a phase of global reorganization and healing. Possible mechanisms of action involving the autonomic nervous system are explored.
INTRODUCTION
The term, Bowen Therapy, is commonly used to describe a number of interpretations of remedial body work that are based on the methods used by an informally trained Australian osteopath named Thomas Ambrose Bowen1 (1916-1982).
The most simplistic interpretations of Bowen Therapy employ standardised sequences of predetermined ‘moves’ to elicit a therapeutic response, while more complex interpretations adopt a more patient-specific approach, whereby interventions are informed by clinical assessment1.
We argue that the integration of holistic assessment methodologies into Bowen Therapy practice offers considerable potential to individualise treatment and enhance clinical outcomes. To this end, we outline a model of holistic tonal assessment consistent with traditional osteopathic principles and informed by the observation and interpretation of craniospinal dynamics.
BACKGROUND
The Dura Mater
The Central Nervous System (CNS), including the brain and the spinal cord, are protected by the bones that make up the skull and the spine. These bony structures are specialised to allow for movement as well as protection. The close relationship between these bony structures and the CNS is mediated and facilitated, in part, by a sensitive connective tissue matrix, which forms a substantial interface between them — a large and extensive fascial structure known as the dura mater2-5.
The outermost layer of the meninges, the dura mater, is a tough protective covering that surrounds the brain and spinal cord. It provides additional support and protection to the CNS, particularly to protect it from mechanical injury. Anatomically, it is firmly attached to the bones of the cranial base (including the occiput, sphenoid, and temporal bones), to the upper cervical regions (particularly C2 and C3), to the sacrum (around S2), and to the coccyx (via the filum terminale)2,3,6. Its fascial nature could be described as extensive and continuous as it merges with the connective tissue sheaths that surround the nerves, muscles, and organs of the body3,6,7,8.
Research has shown that the dura is richly innervated and contains free nerve endings that act as nociceptors and mechanoreceptors, enabling it to detect mechanical deformation, including stretching, pressure, or tension within the meningeal layers9,10. It has been proposed that these signals can contribute to protective reflexes2,11,12 which prompt muscle contractions in nearby structures to protect the CNS.
Due to its anatomical attachments and its neural sensitivity, the dura mater acts as a neuromeningeal interface which monitors the position and movement of the various bony structures to which it is attached. It continually communicates this information to the CNS which responds and adapts accordingly2,6,12. It can be inferred that when a Bowen move or procedure affects the position or movement of any osseous site to which the dura mater is attached, it may induce a functional response within the CNS13.
The Central Nervous System sets the Tone
More than a hundred years ago, D.D. Palmer, the founder of Chiropractic famously stated, ‘Life is the expression of tone. In that sentence is the basic principle of chiropractic’. 14
In his 1927 Chiropractic Textbook, Ralph W. Stephenson explored the idea that tension within the dura mater and spinal cord could lead to neurological dysfunction, potentially resulting in various neurological and musculoskeletal symptoms, as well as other health issues15.
The concept was further developed when the term ‘Adverse Mechanical Tension’ was formally introduced by neurosurgeon Alf Breig in his 1978 publication Adverse Mechanical Tension in the Central Nervous System. In his pioneering work on the biomechanics of the CNS, Breig explored how tension could affect the spinal cord and nerve roots, potentially leading to distant neurological symptoms, and he maintained that the nervous system must be treated as a continuous tract of nervous and supporting tissues16.
Fascial and Neural Continuity
Palmer, Stephenson, and Breig all recognised the extensive fascial and neural continuity provided by the dura mater and they all recognised that restrictions or stress affecting the dura can lead to altered muscle tone elsewhere in the body. These observations form important foundations for numerous schools of chiropractic17,18, osteopathy19,20, and Bowen therapy21, wherein manual therapists assess muscle tone not just locally, but as a reflection of central dural tension.
Biomechanical dysfunction or restriction affecting the sites of dural attachment can generate tensions that spread through the whole dural system8,17,18,22. In the context of chiropractic neurology or craniosacral therapy, such a dysfunction would be viewed as a global lesion and could have the potential to affect neurological flow, cerebrospinal fluid dynamics, and the entire body’s postural tone20,22-25.
The basic premise here is a simple one: structural integrity of the musculoskeletal system contributes to optimum function of the CNS. When this is happening, there will be symmetry of tone on either side of the body. When biomechanical disturbance affects any of the sites of dural attachment it results in the development of asymmetrical tensions on either side of the spine23-25.
Clinically, these tension states can be observed and traced back to their site of origin23-26. In this context, tonal asymmetry becomes a valuable guide to locating and correcting spinal and cranial dysfunction21-25,27,28.
Holistic Tonal Assessment
Holistic tonal assessment involves a systematic approach to evaluating the expression of neurological tone throughout the body. This process is typically conducted through a combination of tactile palpation and visual observation. At its core, Bowen therapy relies on the palpatory assessment that is embedded within each Bowen move. By palpating resting tension states in significant structures, such as biceps femoris, the paraspinal muscle bundles, and the Achilles tendons, clinicians can identify subtle variations in tone that may reflect underlying dysfunction. In most cases, palpatory findings are supported by visual observation (see Figure 1). Developing proficiency in this form of assessment requires specific training to ensure that structural artifacts do not distort the interpretation of tonal patterns.
The assessment is termed holistic because it conceptualises the body’s systems—including the CNS, its meningeal structures, and musculoskeletal components—as an integrated and continuous functional unit. Within this framework, neuromeningeal tension states are understood to be associated with biomechanical disturbances at various dural attachment sites. As such, this method allows for the identification and treatment of dysfunctions not limited to the site of the patient’s symptom presentation but extending to remote, interconnected anatomical regions.
Ongoing holistic assessment provides valuable insights into the multifaceted nature of dysfunction, particularly in complex, multi-layered clinical presentations25,28. Each identifiable layer of dysfunction is regarded as an adaptive response by the body to preserve the integrity of vital structures. Over time, multiple layers of dysfunction may accumulate, contributing to persistent or chronic symptomatology that may manifest across diverse and seemingly unrelated bodily regions8,25,26,28,29.
In relatively uncomplicated presentations involving a single dysfunction site, resolution of the primary lesion typically results in restoration of tonal symmetry. Conversely, in chronic or complex cases, therapeutic intervention at one site may address one layer of dysfunction allowing another layer to emerge12,25. The ability to observe and interpret these transient changes enables the therapist to access deeper, otherwise concealed layers of dysfunction, thereby supporting a more comprehensive, holistic, and effective treatment strategy 23-26,30-32.
In clinic, real-time holistic tonal assessment allows us to recognise three distinct “modes” for the patient:
1. Tonal symmetry – a prevailing state of tonal symmetry is an indication of healthy, balanced neuromeningeal function.
2. Tonal asymmetry – tonal asymmetry is an indicator of dural irritation. It represents a systemic neuromusculoskeletal adaptation and compensatory response, typically arising from a sustained state of dysfunction associated with one or more of the dural attachment sites.
3. The Window of Symmetry – a temporary state of tonal equilibrium that arises following one or more effective therapeutic interventions. This state may persist for several hours, days, or, in some cases, extend beyond a week. Despite its temporary nature, this phenomenon holds significant clinical relevance for practitioners of complementary manual therapies, such as Bowen therapy (see Figure 1).
We propose the transition from a state of tonal asymmetry to temporary symmetry illustrates a measurable shift in how the CNS is responding to neuromeningeal dysfunction. Although the primary dysfunction may remain unresolved, the emergence of this symmetrical state suggests that the CNS has transitioned from a compensatory mode—focused on adaptation and protection—to an integrative or corrective mode, actively engaging in the resolution of underlying dysfunction.
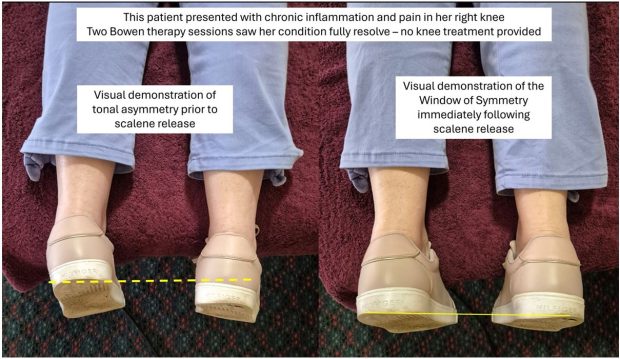
Figure 1: A visual demonstration of tonal asymmetry (prior to treatment) and the Window of Symmetry (following treatment). Note: While an image cannot convey tactile findings, in this instance, palpation revealed increased tension in the left Achilles tendon and the left lumbar paraspinal muscles. This tonal asymmetry responded to a right-sided scalene release.
Clinical Significance of Tonal Assessment
Tonal assessment provides therapists with real-time feedback that can confirm whether, or not, their therapeutic interventions are accurately targeting the primary sites of dysfunction. Careful observation allows therapists to evaluate the effect of any given move or procedure, and to see when treatment is effective and complete2.
In cases involving multiple sites of dysfunction, the CNS response is based on the perceived hierarchy of threat or stress at any given time33. Throughout the course of a treatment, in response to effective intervention, the presentation of tonal asymmetry is expected to change. Once the initial layer of dysfunction has been addressed, additional layers are likely to emerge according to the body’s intrinsic prioritisation2,18,25. Using holistic tonal assessment as a guide, treatment will always be targeted to the primary source of dural irritation at that time.
In addition to guiding treatment and enhancing clinical outcomes, holistic tonal assessment offers other benefits to the therapist.
It enables the early detection and correction of dysfunction states before they become symptomatic. This proactive approach allows therapists to identify and treat subclinical presentations, including subtle dural irritation, and thereby use Bowen therapy to promote function and health2,12.
One of the most significant advantages of this process, however, is the opportunity it offers for continuous clinical learning through real-time feedback. For Bowen therapists, it provides valuable insight into the immediate effects of each move or procedure, allowing ongoing evaluation and comparison of effect. This facilitates the refinement and evolution of therapeutic approaches across multiple areas of practice.2,12,18. Real-time palpatory feedback plays a vital role in enhancing therapists’ perceptual acuity and diagnostic capabilities, ultimately contributing to the development of advanced tactile sensitivity12,21. For manual therapists, including those practicing Bowen therapy, the integration of real-time feedback during patient interactions facilitates continuous professional growth and lifelong clinical development2.
Clinical Significance of the Window of Symmetry
Observation of the Window of Symmetry allows the Bowen therapist to gauge the healing response. It allows us to control therapeutic inputs, to monitor the body’s response to those inputs, and to measure the progress of the therapeutic process. It also informs the therapist about the duration of the resulting healing response. and provides valuable information for patient management, particularly regarding the optimal timing for subsequent interventions. This overall understanding empowers practitioners who seek to restore function and facilitate the body’s innate capacity for self-regulation and healing.
DISCUSSION
Underlying Principles
Traditional osteopathic principles embrace a holistic framework, conceptualizing the body as an interconnected and unified whole. Central to this perspective is the belief in the body’s innate ability to self-regulate and heal, with the practitioner’s role being to facilitate this intrinsic capacity21,29.
These principles are not exclusive to osteopathy; indeed, they are foundational to numerous complementary and alternative health disciplines, including chiropractic, traditional Acupuncture, and Bowen therapy. Philosophical alignment with these principles may help explain why Mr. Bowen identified himself as an osteopath21.
Bowen therapy aligns most closely with these principles when it is guided by holistic tonal assessment and informed by the Window of Symmetry. Within this model, the practitioner is well positioned to support a phase of global reorganization and healing.
Nervous System Response
Bowen therapy acts at an interface between the peripheral and central nervous systems. Although the moves and procedures are applied to somatic tissues, the effects of the input extend, in real time, into the CNS13,35,36. For the therapist, this becomes clearly observable when the patient’s body enters the Window of Symmetry.
Many schools of manual therapy, including Bowen therapy, claim that treatment helps the body to heal itself by evoking a heightened parasympathetic response2,13,18,37. The parasympathetic nervous system is said to have cranio-sacral outflow because its neurons originate in the cranial and sacral regions of the CNS2,3. Since the Window of Symmetry is achieved through targeting dysfunction specifically affecting dural attachment sites, we assert that the Window of Symmetry is an indication of a cranio-sacral response.
Building on this interpretation, we propose that the onset of the Window of Symmetry signifies a physiological transition from a prevailing mode of protection to a temporary mode of correction. We hypothesise that this illustrates enhanced parasympathetic activity which supports the ensuing process of restoration and reorganisation. Furthermore, we assert the enhanced parasympathetic response continues to facilitate changes associated with an ongoing healing process for the duration of the Window of Symmetry.
CONCLUSION
This article supports the notion that the great majority of symptoms seen in the clinic are distant expressions of a central issue and it underscores the importance of a holistic approach to assessment and treatment.
When coupled with an understanding of neuromeningeal dynamics, holistic tonal assessment offers a valuable lens to view layers of dysfunction, to target treatment, and to evaluate therapeutic response.
For practitioners of complementary medicine, the goal of treatment is to restore function at key anatomical and physiological sites, thereby supporting and enhancing the body’s inherent ability to self-regulate and heal. Holistic tonal assessment and the Window of Symmetry serve as powerful tools to support this process. We propose that the Window of Symmetry reflects increased parasympathetic nervous system activity, which is closely linked to the body’s natural healing mechanisms. As such, it offers visual and tactile confirmation of nervous system modulation, making it an unparalleled indicator for guiding and validating therapeutic interventions.
We hope that the foundational concepts of neuromeningeal dynamics, holistic tonal assessment, and the Window of Symmetry described herein will positively influence the way Bowen therapy is taught and practised.
REFERENCES
1. Strachan SM. Bowen therapy today: an 18 April 2014 overview. Bowen Therapy Worldwide; 2014 Apr 18. Available from: https://www.bowentherapy.org.uk/docs/articles/shirley-strachan-report-on-tom-bowen-18Apr14.pdf
2. Chila AG, editor. Foundations of Osteopathic Medicine. 3rd ed. Baltimore: Lippincott Williams & Wilkins; 2011. p. 595–615.
3. Standring S, editor. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. London: Elsevier Health Sciences; 2020. p. 729–732, 776–781, 273–276, 786–788.
4. Snell RS. Clinical Neuroanatomy. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2010. p. 6–12.
5. Enix DE, Scali F, Pontell ME. The cervical myodural bridge, a review of literature and clinical implications. J Can Chiropr Assoc. 2014 Jun;58(2):184-92. PMID: 24932022; PMCID: PMC4025088.
6. Scali F, Pontell ME, Enix DE, Marshall E. Histological analysis of the rectus capitis posterior major’s myodural bridge. Spine J. 2013 May;13(5):558-63. doi: 10.1016/j.spinee.2013.01.015. Epub 2013 Feb 11. PMID: 23406969.
7. Stecco C, Stecco A, Macchi V, Porzionato A, Duparc F, De Caro R. The myodural bridge and its relationship with the dura mater: an anatomic study and consideration of clinical significance. J Bodyw Mov Ther. 2013;17(3):364–9.
8. Schleip R, Findley TW, Chaitow L, Huijing PA. Fascia: The Tensional Network of the Human Body: The science and clinical applications in manual and movement therapy. 2nd ed. Elsevier Health Sciences; 2012. Chapter 7, Dura Mater and Its Fascial Connections
9. Groen GJ, Baljet B, Drukker J. The innervation of the spinal dura mater: anatomy and clinical implications.
Acta Neurochir (Wien). 1988;92(1-4):39–46.
Available from: https://link.springer.com/article/10.1007/BF01401971
10. Elbadawi M, Alshorman A, Alawneh K, Abu Khdair W, Al-Nusairi A, Alomari R.
Dura mater: anatomy and clinical implication. J Behav Brain Sci. 2021;11(4):104–123.
Available from: https://www.scirp.org/pdf/jbbs_2021093015161884.pdf
11. Bergmann TF, Peterson DH. Chiropractic Technique: Principles and Procedures. 3rd ed. Mosby (Elsevier); 2010.
12. Greenman PE. Principles of Manual Medicine. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2003.
13. Wilks J, Knight I. Using the Bowen Technique to address complex and common conditions. London: Singing Dragon; 2014.
14. Palmer DD. The Chiropractor’s Adjuster. Davenport, IA: Palmer School of Chiropractic; 1910.
15. Stephenson RW. The Chiropractic Textbook. Davenport, IA: Palmer School of Chiropractic, 1927.
16. Breig A. Adverse mechanical tension in the central nervous system: an analysis of cause and effect—relief by functional neurosurgery. Stockholm: Almqvist & Wiksell; 1978.
17. Shriner S. A review of Torque Release Technique. Ann Vertebral Subluxation Res. 2012 Jul 12:72–6
18. Kent C. Models of vertebral subluxation: A review. J Vertebral Subluxation Res. 1996;1(1):1–7.
19. Jäkel A, von Hauenschild P. Therapeutic effects of cranial osteopathic manipulative medicine: a systematic review. J Osteopath Med. 2011 Dec;111(12):685–93. doi:10.7556/jaoa.2011.111.12.685.
20. Zweedijk RJ, van Oosten D. Osteopathy in the cranial field: from a systems theory perspective. J Altern Complement Integr Med. 2021;7:197. doi:10.24966/ACIM-7562/100197.
21. Pennington G. A Textbook of Bowen Technique – A comprehensive guide to the practice of Bowen therapy. Barker Deane Publishing, 2012
22. Ferguson AJ, McPartland JM, Upledger JE, Collins M, Lever R, Cranial Osteopathy and Craniosacral Therapy: Current Opinions. J Bodyw Mov Ther. 1998 Jan;2(1), 28-37
23. Nadler A, Holder JM, Talsky M, Torque Release Technique – A Model for Chiropractic’s Second Century. Canadian Chiropractor Feb 1998 Vol 3, (1)
24. Hodgson N. The role of the spinal dura mater in spinal subluxation [unpublished manuscript]. 2008. Available from: https://www.superhealthy.com.au/post/torque-release-technique-all-the-research
25. Fletcher DM, A Tonal Solution for Subluxation Patterns – Torque Release Technique Analyses Cranial-Spinal Meningeal Functional Unit. Canadian Chiropractor April 2004, Vol. 9, No. 2.
Available from: http://efaidnbmnnnibpcajpcglclefindmkaj/https://www.torquerelease.com.au/Tonal-Solution-For-Subluxation-Patterns.pdf
26. Senzon S, Epstein D, Lemberger D. A Historical Perspective on Network Spinal Analysis Care: A Unique Insight into the Spine’s Role in Health and Wellbeing. Chiropr J Aust. 2017 Dec 1;45(4):304–23. Available from: https://www.cjaonline.com.au/index.php/cja/article/download/176/76
27. Becker D, Theodossis C, Schwartzbauer M, Brewster A. Technique protocols for evaluating supine functional leg length inequality: comparison of two technique protocols using the cervicocephalic kinesthetic sensibility test as a standard measure. J Upper Cervical Chiropr Res. 2025; March26 6–15.
28. Senzon SA, Green BN. The neurophysiological basis for chiropractic care in chronic pain management. J Chiropr Med. 2013;12(1):21–9. doi:10.1016/j.jcm.2013.01.002.
29. Still AT. Philosophy of Osteopathy. Kirksville, MO: American School of Osteopathy; 1899.
30. Fryer G. Somatic dysfunction: An osteopathic conundrum. Int J Osteopath Med. 2016;19(1):1–8. doi:10.1016/j.ijosm.2016.02.002.
31. Licciardone JC, Kearns CM. Somatic dysfunction and its association with chronic low back pain, back-specific functioning, and general health: Results from the OSTEOPATHIC Trial. J Osteopath Med. 2012;112(7):420–428. doi:10.7556/jaoa.2012.112.7.420.
32. Arcuri L, Consorti G, Tramontano M, Petracca M, Esteves JE, Lunghi C. “What you feel under your hands”: exploring professionals’ perspective of somatic dysfunction in osteopathic clinical practice—a qualitative study. Chiropr Man Therap. 2022;30:32. doi:10.1186/s12998-022-00444-2.
33. Melzack, R. From the gate to the neuromatrix. Pain, 1999; Supplement 6 (June 1999): S121–S126
34. Epstein DM. Network Spinal Analysis: a system of health care delivery within the subluxation-based chiropractic model. J Vertebral Subluxation Res. 1996;1(1):1–9.
35. Pickar JG. Neurophysiological effects of spinal manipulation. Spine J. 2002;2(4):357–71. doi:10.1016/S1529‑9430(02)00400‑X.
36. Herzog W. The biomechanics of spinal manipulation. J Bodyw Mov Ther. 2010 Jul;14(3):280–6. doi: 10.1016/j.jbmt.2010.03.004.
37. Whitaker JA, Gilliam PP. A gentle hands healing method that affects the autonomic nervous system as measured by heart rate variability and clinical assessment.
USA: American Bowen Academy; c2001.