Bowen Technique Case Studies 79 – 84
Case 79: Treatment of a patient with Post Concussion Syndrome
Mark (37 years old) presented to the clinic with a nine-month history of a constant headache, dizziness, nausea, and tinnitus, as well as frequent migraines and daily episodes of vertigo. These symptoms followed a fall nine months earlier which resulted in concussion with a loss of consciousness. His medical specialists had labelled his condition “post concussion syndrome”.
The Mayo Clinic explains that post concussion syndrome occurs when symptoms of mild traumatic brain injury last longer than expected. It states the main symptoms of the syndrome include headache, dizziness, tinnitus, and problems with concentration and memory.
For the past nine months, Mark had been having regular physiotherapy and chiropractic treatment yet his symptoms had persisted and he has been unable to return to work as a school teacher. He was recently referred to our clinic by his neighbour.
Assessment in the prone position revealed a left-sided dural drag (about 2 cm) and while the screening was negative for neck involvement, it did show positive for sacroiliac joint dysfunction.
I applied the Lower and Upper Back procedures and then had him turn supine so I could assess the state of the upper dural attachments. Using the moves of the Neck procedure, I was able to recognise that his neck felt quite ‘normal’. I checked his jaw and his sternocleidomastoid muscles and found these were also unremarkable. On the basis of these observations, I knew his issue was not directly related to dysfunction in the region of the head and neck. At this point, I became confident that his symptoms must be resulting from coccyx dysfunction.
In order to correctly assess coccyx dysfunction, I feel it is imperative that any pelvic issues are first identified and resolved. In Mark’s case, I checked and released his adductors which were very tense and tender and then had him turn prone once again.
On returning him to the prone position, it was evident that he now showed a right-sided dural drag. I tried using a Reverse Coccyx procedure but nothing changed so I applied a Regular Coccyx correction. As I made contact with the lateral margin of the coccyx, it became clear that this site was extremely sensitive to any pressure. I talked Mark through the pain and completed the procedure using the right leg as the lever and then I let him rest for five minutes. After the rest period, he showed perfect symmetry.
I told him his physiotherapist and his chiropractor had done wonders with his neck but that his main issue all this time had actually been his tailbone. I told him it would take a few treatments but that we should be able to resolve all his symptoms over the next four or five weeks.
At the follow-up treatment a week later, Mark told me the first few days following the treatment had been very difficult as many of his symptoms seemed to have temporarily intensified, however, they then began to settle and over the last two days he was feeling a lot better. I repeated the same treatment and noted the target sites were far less tender than they had been the week prior.
Mark came for his third session one week later and he was excited. He told me the nausea and dizziness had gone away. He said he had not experienced any migraines and that his headache had reduced to just a dull sensation. He could still hear the tinnitus but it too had reduced in intensity.
I continued to assess and address his coccyx on a weekly basis for another three sessions and over that time all of his symptoms completely resolved. Mark reports that for the last two weeks he has been feeling 100%. He has been cleared to return to work and he is in the process of coming off all his medications.
Comment: This case illustrates the importance of holistic assessment as well as holistic treatment.
Mr Bowen understood and embraced the holistic nature of the central nervous system. He assessed the spine as a whole and he therefore assessed the coccyx as a standard part of his approach to every treatment. Empowered by appropriate holistic assessment, we can target our treatments accordingly.
The mainstream medical world embraces a reductionist, evidence-based view and does not recognise the relationship between the coccyx and cranial function. Sadly, the alternative professions that pioneered the holistic approach (Chiropractic and Osteopathy) now seem to have abandoned it in favour of the “evidence-based approach”. Presumably, this has made their training more credible. Perhaps patients like Mark pay the price for their new-found credibility.
Case 80: Treatment of Achilles tendonitis
Mena, a very fit and active 80-year-old, came to the clinic two weeks ago complaining of severe pain in her Achilles tendon just above its attachment at the right heel. She also complained of generalised swelling and pain in her right ankle. The symptoms had come on gradually and she couldn’t recall any incident that may have resulted in an injury to the area however the pain had prevented her from walking any distance for at least a month. She had received some physiotherapy and some massage but had experienced no relief.
On assessment in the prone position, her left leg appeared to be about two centimetres shorter than the right. With her head turned to the right, however, the leg lengths appeared to be equal (positive cervical turn test). I told her she had a neck problem.
After running through the Lower and Upper Back moves, I turned her over and began to work on her neck. The scalenes on the right side were tense and sore and I released them over several minutes. I then began to palpate the right calf but as I began to move the upper part of the tendon Achilles she tensed in anticipation of pain. She said she was afraid of me touching the inflamed area. I told her I thought we could fix it without working directly on the Achilles tendon and so I had her turn prone again to see if she showed symmetry.
She still showed a short left leg but only about one centimetre this time. I applied a coccyx correction (reverse coccyx procedure) and this resulted in a return to a state of symmetry. I asked her to return in a week for another treatment.
Mena returned for the follow-up treatment (last week) claiming she was at least 95% better. The swelling and pain had gone from her ankle and the Achilles was no longer sore to touch and she could walk without discomfort. I assessed her and noted that she still held symmetry. I assessed her neck and it felt quite normal. I suggested she come once more in a week, just to check the treatment was holding.
She came back again today, and she was delighted. She declared that her foot felt “perfect”, and she happily told me she felt like a 40-year-old again! I asked if she was impressed that I had fixed her without working on the ankle or the Achilles tendon and she shook her head. “No”, she said. “That’s your job! I just expect you to fix me – I don’t care how you do it!”
Comment: Another case that illustrates the importance of holistic assessment as well as holistic treatment. In clinical practice we commonly find the underlying primary dysfunction far from the presenting symptoms. To quote the great Ida Rolf, “Where you think it is, it ain’t”.
Case 81: Recurrent episodes of paresthesia in the right arm and right leg
Rex (83 years old) came to the clinic three weeks ago complaining of frequent episodes of “pins and needles” (paresthesia) in his right arm and his right leg. He had been experiencing the right-sided paresthesia for more than three months, typically suffering four or five episodes each week. The symptoms often came on in the evening, while he was watching television, and the pins and needles and numbness would come into in his right arm (extending down into his hand) and in his right leg (including his thigh and his knee). Medical investigations, including an MRI scan of the brain, had so far failed to determine any identifiable pathology and he was now scheduled to see a neurologist.
I assessed him in the Prone position and noted a right -sided dural drag that made the right leg look about 15mm shorter than the left. Screening was unremarkable so I began the treatment with the Lower and Upper Back procedures and then had him turn supine. As I performed the moves of the Neck Procedure, I noted that his scalenes were normal but there was significant tension at the site of Move 6, in the paraspinal bundle on the right side of the neck.
I checked the tension of the sternocleidomastoid muscles and was pleased to find great rigidity and tenderness associated with the muscle on the right. The muscle on the left felt quite normal. Rex wasn’t too pleased with the moves I was making on his right sternocleidomastoid but I assured him it was all good news. Using a model of the cranial bones, I explained how this tension was putting a strain on the temporal bone and that this might be the reason he was experiencing these odd symptoms. I treated the suspect muscle several times over a ten-minute period and it released nicely.
I turned Rex prone once again and noted that he now showed symmetry. I asked him to return for a follow-up treatment in a week.
Rex returned for the follow-up treatment saying he had not experienced any episodes since the treatment. On assessment, he still showed symmetry and, during the treatment, the only issue I noted was very slight tension in the right sternocleidomastoid.
Rex returned to the clinic again yesterday (two weeks since the second treatment) and he was very happy. He no longer experiences any episodes of pins and needles, or numbness, and he feels his whole body has become looser and freer. He maintains symmetry and the sternocleidomastoids are both loose and happy. He no longer has any abnormal tension in his neck and I told him that no further treatment is required.
Comment: For the therapist, this case seemed quite simple and straightforward. For the patient, the symptoms were not debilitating, yet their persistent recurrence had raised grave concerns as to possible underlying pathologies. This patient (and his doctor) had been initially concerned about potentially serious brain pathology and then about the possibility of serious degenerative neurological conditions. The relief the patient experienced following a simple muscle release went far beyond the recovery from the pins and needles and numbness.
Case 82: Treatment of severe hip pain in a 90-year-old male
With the aid of a walking frame, Fred, who is 90 years old, slowly limped along the corridor and into the treatment room. With a wounded and sad expression, he told me he was experiencing severe pain in his left hip and that the pain was shooting into to his lower leg with every step he took. The pain had been relentless for the last two months and he was deeply concerned because he had become dependent on pain killers. I asked him if he could lie face-down on my treatment table and, although it was a somewhat difficult task, he did.
With Fred lying prone, a left-sided dural drag was easily observed – it made his left leg appear at least 4 centimeters shorter than the right (see the pictures below). I should mention at this point that I had treated Fred about two years ago and, at that appointment, he had presented with perfect symmetry. I conducted a thorough assessment, but all the screening tests were unremarkable.
I gently worked through the moves of the upper and lower back procedures and then had him turn over on to his back. In the supine position, he still showed a short left leg of around 4 centimeters. I checked his neck, but it felt fine.
In recent times, I have been particularly interested in the presentation of the dural drag as the patient moves between the prone to supine positions. When the patient moves from prone to supine, a short left leg (in the prone position) can present as either a short left or a short right leg in the supine position. I have coined the terms “Switcher” and “non-Switcher” to describe the patterns observed. (The term “Switcher” means the short left leg observed in the prone position changes to present as a short right leg in the supine position. If the left leg is observed to be short in both the prone and supine positions, then the pattern is described with the term, “non-Switcher”.
Since Fred demonstrated the short left leg in both prone and supine, I noted that he was a non-Switcher. I have found this to be an observation with certain clinical significance. The non-Switcher presentation points to dysfunction in three possible places, i.e., the abdominal external oblique on the short leg side, the adductor on the short leg side, or the coccyx.
I checked the left abdominal external oblique and the left adductor but I found nothing abnormal, so I concluded the primary issue was coccyx dysfunction. I asked Fred to turn over once more so I could address the coccyx.
Using the left leg as the lever, I applied a Reverse Coccyx procedure but nothing changed. I then tried a regular coccyx procedure using the left leg as the lever but still there was no change. I was quite certain the coccyx was the primary issue so I decided more effort was required on my part. I repeated the Reverse Coccyx procedure but this time I maintained quite a long and firm challenge with the leg at its end range (perhaps 4 or 5 seconds) and I was rewarded with a sad moaning sound from Fred as I did so. I let him rest for five minutes before taking a final photograph of the resulting symmetry.
As Fred walked back up the corridor to reception, he commented that pain appeared to have improved significantly. He told me the shooting pain was no longer happening as he walked.
One week later, Fred returned to the clinic a very happy man. Although he still walked with the aid of his walking frame (he said it was to help with his balance) he claimed he was at least 90% pain-free. He had stopped taking his analgesic medications and he felt at least 10 years younger.
Comment: The most interesting aspect of this case study is that the initial Coccyx procedure failed to restore symmetry. Based on palpatory findings throughout the treatment, and on the observation of the non-Switcher presentation, I reasoned that I was working in the right place but that my technique had been ineffective. I repeated the procedure using different levels of input and was appropriately rewarded.


Case 83: Treatment of chronic shoulder and elbow pain
Andrew presented to the clinic complaining of chronic shoulder pain. He described a slow and steady onset of pain in his right shoulder that had now been constant for more than six months. It was gradually getting worse and had begun to interfere with his ability to participate in competitive target shooting events. Further enquiry revealed that certain actions could cause brief episodes of severe pain in his right elbow.
I assessed Andrew and found that he showed good tonal symmetry. I commenced treatment with the Upper Back and Neck Procedures and found these sites all felt quite ‘normal’. I decided his problem had to be associated with local structures in the shoulder and elbow, so I began to assess these areas, one muscle at a time. There was general soreness in several places, including the infraspinatus, the biceps, and the common extensor tendon, but (based on my palpation) nothing stood out as the likely source of the trouble.
I had Andrew sit on the edge of the table so I could perform the Shoulder Procedure. The left shoulder first (which felt quite normal), and then the right…
Palpation is such an important part of our work. As I positioned my thumbs under the posterior border of the right deltoid, I noticed a hard edge in the tissues beneath the deltoid. I changed the angle of the move to go more deeply into the back of the shoulder, so I could apply a better challenge to the hard ridge of tissue. At that point, Andrew’s facial expression changed. His eyes widened and he told me he could feel the pain all the way down to the elbow. With this extra encouragement, I completed the move, through the deltoid and over the lateral head of the triceps, and then stood back to enjoy Andrew’s reaction.
Although the move had been very uncomfortable, he knew I had found the place that his pain was coming from. I treated Andrew a total of four times (each treatment was two weeks apart) and at each visit he reported significant improvement. At each session, I was able to feel a significant reduction in the hard edge in the triceps. By the fourth visit (yesterday) he was pain-free and fully functional, and I could no longer palpate any abnormality in the triceps tendon.
Comment: This case highlights the importance of palpation as an assessment tool. It also encourages us to look at the different ways any single move may be used in order to direct its effect.
In the book, I discuss Move 1 of the Shoulder Procedure (p. 176) and I state, “…Another significant point to make is that the pressure can be applied in different directions when executing this move. The option to focus primarily on the deltoid sees the therapist positioning the thumbs under the posterior border and moving upwards toward the patient’s ear. Sometimes a better effect is achieved by directing the move “inwards” to provide greater stimulation to the teres and triceps.
Most students are taught that an effective move is one which generates a twitch response that can be felt in the triceps tendon at the elbow. Directing the pressure of the move “inwards” certainly generates a much stronger triceps twitch response.”

Case 84: Treatment of ongoing neurological dysfunction including headache and loss of the sense of smell
Charlie (51 years old) came to the clinic ten weeks ago complaining of a chronic headache, neck pain, and general stiffness. In addition to these primary symptoms, he also suffered from poor balance and the complete loss of his sense of smell and taste. He stated that he had been perfectly fit and healthy until an incident eight years prior, when he was struck in the head with a cricket ball. The injury resulted in immediate loss of consciousness and the loss of his left ear. He was subsequently diagnosed with a traumatic brain injury, and, despite a rigorous rehabilitation program that spanned twelve months and involved numerous different therapies, he has continued to suffer ongoing pain and neurological dysfunction and impairment.
I asked Charlie to lay prone on the treatment table so I could conduct my initial assessment. A visual check of his leg-lengths showed an initial presentation of “symmetry” so I commenced the treatment as I always do, with the Lower and Upper Back Procedures, and then had him turn supine so I could move on to his neck. The paraspinal bundle on the left side of the neck was much tighter than the one on the right. I checked his sternocleidomastoid (SCM) muscles and found the one on the left side was much tighter (and far more tender) than the one on the right. Using firm, slow moves, I “gently” released the left SCM (I knew when it had released because I was able to palpate the subsequent release of tension in the left paraspinal bundle).
I had Charlie turn prone again and conducted another quick assessment of symmetry. This time, his right leg was considerably shorter than the left. Using the right leg as a lever, I conducted a beautiful reverse coccyx procedure. This left Charlie nicely balanced, so I concluded the treatment and asked him to come back in a week or two for a follow-up.
I have treated Charlie on five occasions since that first treatment. He has been coming regularly for fortnightly treatments (since that’s all his budget will allow). The treatment has basically been the same each week, and the target tissues have responded nicely over time. Each week I work on the SCM and then check and correct the coccyx. On one or two occasions, I also worked on his TMJ, and once on his right biceps.
In the first month, the headache and the neck pain completely resolved. Charlie told me he thought he would have that headache for the rest of his life. The generalized stiffness resolved, and he began to feel that his balance had become perfectly normal too. He even commented that his golf game had improved dramatically. He asked me if I thought his sense of smell and taste might improve and I told him I thought that was a long shot and that I wouldn’t count on it.
I saw Charlie yesterday (10 weeks since we started the treatments) and he was grinning from ear to where his other ear should have been. I asked why he was looking so happy, and he cheekily replied, “because you were wrong”.
“About what”, I asked?
“I can smell things”.
He told me he was in a friend’s garden and was shocked that he could smell the daphne. He then found he could smell other flowers too. And then at work his mates thought it was hilarious when he complained about the smell of the septic overflow. He told me he is feeling great, and that his golf handicap had fallen from 13 to 10 since we started the treatments.
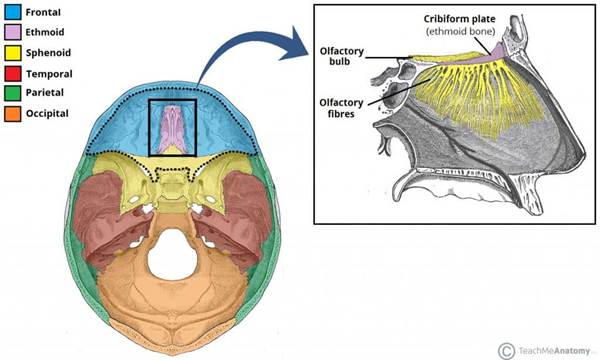
Comment: Targeted directly to specific sites associated with prevailing neuro-meningeal stress, certain Bowen procedures can have a profound impact on the function of the cranial base and the cranial dura.
The olfactory nerve (the first cranial nerve) is responsible for our sense of smell. It passes from the cranial vault through the cribiform plate of the ethmoid bone. To make this transit, it must also pass through the layers of the dura. In this case, resolution of dysfunction at dural attachment sites (temporal bone, sphenoid bone, occiput and coccyx) has facilitated systemic change in meningeal tension and function, resulting in resolution of the patient’s chronic symptoms.
This case study shows how simple and effective Bowen therapy can be when it is appropriately targeted and applied.